Some of the risk factors that may restrict the natural growth of your baby’s skull include:
- Premature birth
- Congenital muscular torticollis (a tilting and/or turning of a baby’s neck to one side as a result of a muscle strain)
- Multiple births (twins, triplets, etc.)
- Restrictive positioning during pregnancy
- Trauma at birth
- Cervical spine abnormalities
- Favoring one side over another
Plagiocephaly: Four Common Head Shapes
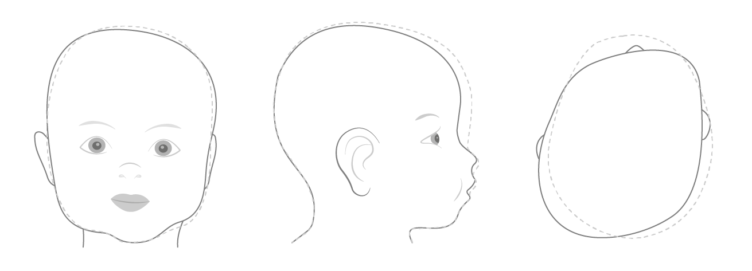
Plagiocephaly, or “flat head syndrome,” is the most common form of cranial asymmetry and is usually identified by a flattening on one side of the back of the head. It is sometimes referred to as a parallelogram shape, because it looks like one side of the baby’s head has been pushed forward.

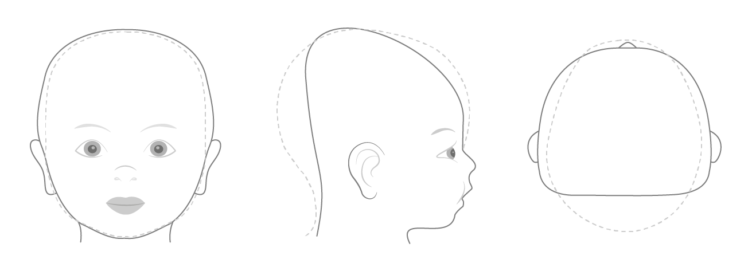
Brachycephaly generally appears as flattening across the back of the head with a prominent forehead, widening above the ears, and the height of the baby’s head may appear taller.
Asymmetric brachycephaly is a combination of plagiocephaly and brachycephaly. It causes a baby to have flatness across the back of their head, which is worse on one side than the other. The baby’s head will also look wide from side to side, compared to the length.
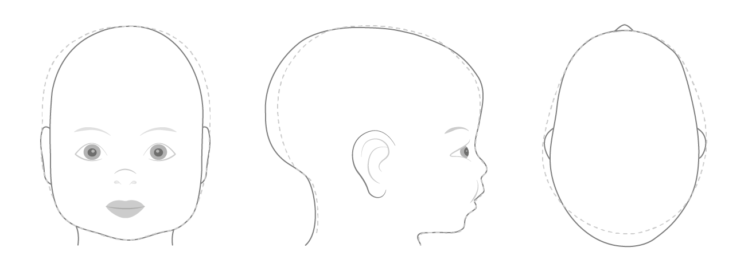
Scaphocephaly is typically observed as a long, narrow head shape. It is commonly seen in premature babies who spent time in the NICU or consistently rest on either side of the head.
How to Identify an Asymmetrical Head Shape
While no child (or adult) has a perfectly symmetrical head, there are ranges of normal development. The majority of cranial asymmetries will correct on their own during the first weeks of life. However, a head shape that is not getting better, or may be getting worse, should be evaluated.
One of the best ways to look for asymmetry is to look at your baby’s head from above (the bird’s eye view) while his or her hair is wet. Also look for red creases on one side of your baby’s neck as they may result from his or her head being cocked to one side, which may be a sign of torticollis.
If you notice any irregularities, schedule an appointment with your child’s pediatrician or physical therapist and ask for a referral to Hanger Clinic for a free evaluation. Whether your baby needs some extra tummy time, repositioning, or helmet therapy, there is a lot that can be done to correct the asymmetry.
1. Lin RS, Stevens PM, Wininger M, Castiglione CL. Orthotic Management of Deformational Plagiocephaly: Consensus Clinical Standards of Care. The Cleft Palate-Craniofacial Journal. 2016;53(4):394-403. doi:10.1597/15-007
A child with arthrogryposis may see a physical or occupational therapist for stretching exercises and may also see an orthotist, a specialist who designs leg braces to help manage their condition.
Orthotic treatment (bracing) can be tailored to a child’s specific needs to help them reach their goals. Bracing may be used to increase joint mobility or to prevent the recurrence of joint tightness. A brace (orthosis) may be prescribed for either daytime and/or nighttime use. A daytime brace can be used to support part of the body or make activities easier. A nighttime brace can be used to provide a stretch to improve joint range of motion. If a child’s joint tightness is severe, surgery may be recommended to improve their function.
1. Kowalczyk, B, Felus, J. Arthrogryposis: an update on clinical aspects, etiology, and treatment strategies. Arch Medi Sci. 20016, Feb 1. | 2. Bartonek, Å. The use of orthoses and gait analysis in children with AMC. J Child Orthop 9, 437–447 (2015). ttps://doi.org/10.1007/s11832-015-0691-7.